
Can you overfeed a baby?

The simple answer is yes, you can! Of course you can. Like all stages of life, biology gifts us with a digestive system which has certain parameters that we are advised to live within in order to stay healthy, comfortable and not become obese. A newborn and infant are no exception within nature’s make-up of this. However, gravely, a large proportion of feeding practices that are commonly taught to parents in the Western World are creating havoc on newborn and infant health, teaching parents to overfeed their newborn or infant beyond their natural capacities and capabilities. Quite frankly, this madness of thinking and teaching needs to change to benefit our young!
At every other age of life we talk about obesity and yet in the first year of life, when our cells and neurons are developing at such a pace, we honour obesity. We say the rolls on arms, wrists and legs are cute and adorable. We boast about baby’s huge weight gains, in the meantime we might be nursing them around the clock because they won’t sleep for long periods and are highly unsettled – all the time being told this is normal and/or baby is just going through a growth spurt or a sleep regression. But all of this is anything but normal. Add to this that parents are sometimes congratulated by well-meaning but misinformed health professionals for large weight gains, and understandably the parent then becomes less likely to query the gain.
What causes baby obesity
- placing baby to the breast, or feeding a bottle if they look to suck or mouth for food. This teaching completely overlooks a newborn and infants innate mechanism of looking to suck for comfort alone - not for food. Sucking is their natural tool to self-sooth. Sucking without food turns on their parasympathetic nervous system, aiding healthy digestive processes. Learning how to read a baby's Six-Wind-Cues and how their basic digestive function operates can help parents differentiate between hunger and the need to suck for comfort.
- cluster feeding in the early afternoon or evening. Many parents are told this is 'normal', or at least that's what parents get taught along with baby is just asking for more at these times, that's why they are upset, and they have 'the witching hour', which is also 'normal'. Each time I hear this I feel my insides coiling up and a huge amount of overwhelming sadness for our newborns that are innocently born into a world where their crying and screaming is labelled as normal! How did we even get to that? Cluster feeding is not normal - it is part of the problem. My clinical research and results with family's time and time again keeps showing me this. You can also read more about the questionable research that so called 'backs' this form of feeding here.
More causes after the FREE Ticket to my Coaching Sessions in my community advert...

- to feed baby from both breasts in one sitting. Unfortunately, this automatically has a baby feeling the effects of lactose overload, and because of the discomfort caused by this (and any discomfort felt by them anywhere in their body) your baby may actually look to suck more often to self-sooth, thus lending weight to the assumption that baby is hungry so feed more.
- that you can't overfeed a breastfed baby, never de-latch a breastfed baby because they will know when they are full, and/or it's possible for baby to suck from a breast and not get any milk, called non-nutritive sucking. These teachings actually, completely contradict basic early biology. Firstly, it takes around 20 minutes for the full satiety levels to be realised by the brain so baby cannot choose when they are full at the time. Secondly, babies don't choose, they react with reflexes and if you go to pull your nipple, or a teat out of a baby's mouth, they will often go to suck it back in and/or suck harder because this is how the reflex works. The same applies if you put anything near the baby's mouth. Thirdly, breastfeeding is a demand and supply relationship. If baby is sucking, then you are providing some milk. Yes, the strength of suck will determine how much, but given the child is often feeling overloaded in the digestive tract from too much food, mother's breastfeeding diet, or lack of winding, they will often suck strongly in reaction to this, wanting to self-sooth rather than because they are hungry. Thus, their discomfort can have them overfeeding - being fed well beyond the size of their stomach and what their innate digestive processes can handle.
Read about the effects of the above after the BabyCues Feeding Volumes & Weight Guide...
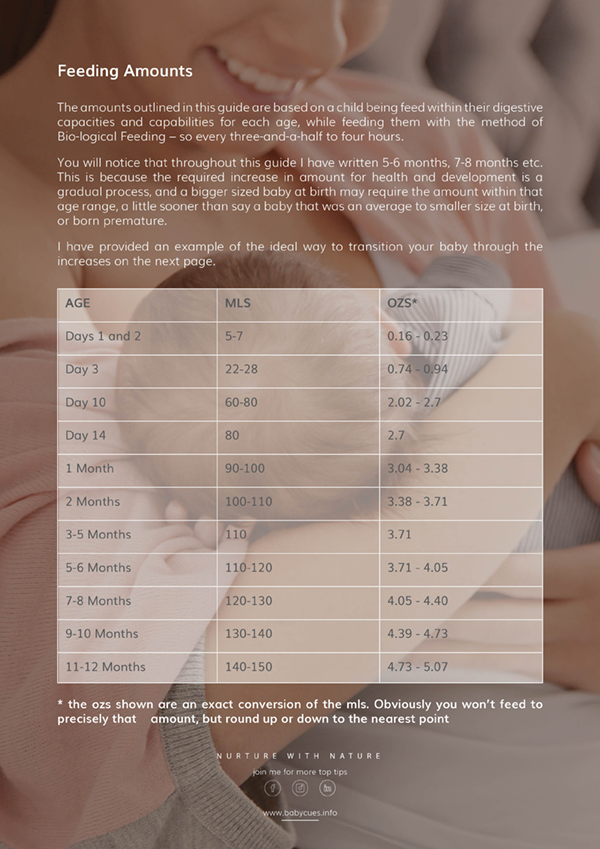
Feed baby to physiological capacities
This BabyCues Guide outlines the amounts to feed a newborn and infant, up to one year of age, when nurturing with BabyCues Bio-logical Feeding methods, which means feeding baby every three-and-a-half to four hours, thus working alongside our children's natural digestive function.
- foster digestive health
- feed to natural capacities
- Reduce Digestive Overload Symptoms
nurture naturally
- foster digestive health
- feed to natural capacities
- Reduce Digestive Overload Symptoms
Effects of overfeeding
Unfortunately for our newborns and infants, the effects of overfeeding are immense. It can cause:
- reflux, or what I call Digestive Overload, the cause of reflux – your baby’s stomach size can only hold certain amounts at each age and it does not have the ability to stretch like an adults, so if there isn’t enough room then it’s more than likely going to come back up.
- colic, or what I call Digestive Overload, the cause of colic - colic is simply caused by an overloading of the digestive system whether it be by gas, diet or the amount of food being received, or tongue and lip tie. When we stop overloading a newborns digestive system, we stop these symptoms. Colic and reflux (Gastroesophaguel Reflux) does not have to exist.
- milk and food being pushed out of the stomach and onward in the digestive tract before it has been appropriately absorbed – newborns and infants do not have the ability to hold onto food in the stomach if there is too much. Instead the amount consumed directly determines how fast that food is pushed through the system, leaving fat globules to abnormally pass out of the stomach and travel through the intestines, lactose to ferment in the duodenum and cause more gas, food particles to potentially pass through the intestinal wall, all of which and more leads to an unsettled child and sometimes the diagnosis of Digestive Overload.
- an increase of hydrochloric acid in the stomach – hydrochloric acids helps a baby breakdown their milk, and the more milk they have the more acid the stomach produces, which irritates the lining of the stomach. The continual overabundance of this can also produce refluxing that smells acidic, which often results in baby being prescribed detrimental H2 blockers and Proton Pump Inhibitors that reduce, or turn off the acid in the stomach, something that is required for healthy digestive function and health. A backward approach to the problem when all we need to do is nurture baby with feeds that are conducive to their natural stomach capacities and capabilities.
- abdominal distention – whereby the stomach is ballooned outward, beyond the girth of the waist and stomach placing pressure on the skin and organs.
- early linear growth – according to Dr Steven Schwarz, a professor of paediatrics at Suny-Downstate Medical Centre, “You can actually drive early linear growth by overfeeding. If the child is growing along the 50th percentile for height and 90th for weight that at least raises a concern.”
- a higher likelihood of developing ‘non-communicable diseases like diabetes and cardiovascular diseases at a younger age. Many co-morbid conditions like metabolic, cardiovascular, orthopaedic, neurological, hepatic, pulmonary, and renal disorders are also seen in association with childhood obesity.’1
- a higher mortality rate in adulthood – long-term epidemiological studies have found childhood obesity to be associated with 50-80% higher mortality in adulthood, predominantly related to cardiovascular disease2,3
The first year of life is a time of exponential development - it is paramount that within our talks about child obesity and our preventative intervention strategy, that newborns and infants are considered! Please feel free to share this blog far and wide to help our young and thanks in advance for doing so.
References
- Sahoo K; Sahoo B; Choudhury AK; Sofi NY; Kumar R; Bhadoria AS; Childhood obesity: causes and consequences, US National Library of Medicine
- Inserm Collective Expert Reports; Childhood obesity; Screening and prevention; 2000
- New Zealand Ministry of Health; An analysis of the usefulness and feasibility of a population indicator of childhood obesity; 2006